Community support groups facilitate health care of older persons (2022 onwards)

ARTH has helped create community support groups for older persons, which have been named Buzurg Milan Samooh. These are groups consisting of older persons in a specific hamlet of the village, aged 50 years and above. The thought behind creating such groups is that several older persons in rural areas face increasing loneliness and isolation as their mobility becomes restricted, families turn nuclear and resources to travel and meet decline. The group serves as a platform for them to meet and socialize, to share problems or common issues and to seek support from similar others in working out a solution. It also enables ARTH to share and better deliver preventive health care and nutrition interventions, to link older persons to its primary health care camps and clinics, and to support referral for investigations and specialised treatment in the city, should that become necessary. Each of these meetings is conducted once a month and is facilitated by ARTH’s field staff. In the 1st meeting, most people are quiet and reserved, as they are not sure what the meeting is about. Field staff present in the meeting explain to them the reason for organizing it, while also pushing them to speak and express themselves. By the 3rd meeting of the group, people express themselves a lot better and have discussions on various topics – their daily lives, how things were before when they were young, their eating habits, etc. They are also encouraged to sing songs and tell stories, the main goal being that by the end of the meeting they feel happier and socially closer to each other. By September 2023, 109 older persons’ support groups have been created in 8 blocks of southern Rajasthan and their experience is being monitored. Issues like old age and widow pensions, health problems and the availability of subsidised grain have already come up during conversations. Problems related to sustaining health, nutrition and wellness (a significant proportion of older persons are undernourished) and digital access to pensions are numerous, but a beginning has been made and older persons now have a group to belong to.
Raahat: Relief and recovery from COVID pandemic in southern Rajasthan (2021-2023)

The second wave of the COVID-19 pandemic highlighted the need for greater preparedness at community level. Even after the pandemic had ebbed, the impact of the pandemic and lockdown on the community was still visible. Despite several relief activities, there were still marginalized and vulnerable sections of the community, like poorer families migrating for work and older persons, who require continuing support to overcome pandemic effects and normalize their daily life. ARTH implemented an intervention to reach out to such vulnerable sections in southern Rajasthan, and to assist them in recovery. Major activities: Since the inception of the programme in September 2021, we identified and located the vulnerable families, and carried out targeted relief activities for these vulnerable families and successfully distributed ration kits, walkers, walking sticks, solar powered lamps, clothes and conducted health care camps in remote rural areas mostly treating people with long-term illnesses which require continuous care and treatment. After the withdrawal of the pandemic, we gradually shifted our focus towards health care for older persons and management of malnutrition among children. Such people were identified and referred to our health camps which take place at a pre-decided location every month. At this camp, a doctor with a camp counsellor is available for the day. This is where older persons and malnourished children along with anyone else who visits the camp are treated. People with long-term illnesses are advised by the doctor to visit again. Some people who present with health complications which cannot be treated at the camp are also referred to the district hospital for further care and treatment.
Monthly rural health camps for older persons and chronic conditions (2020-2024)
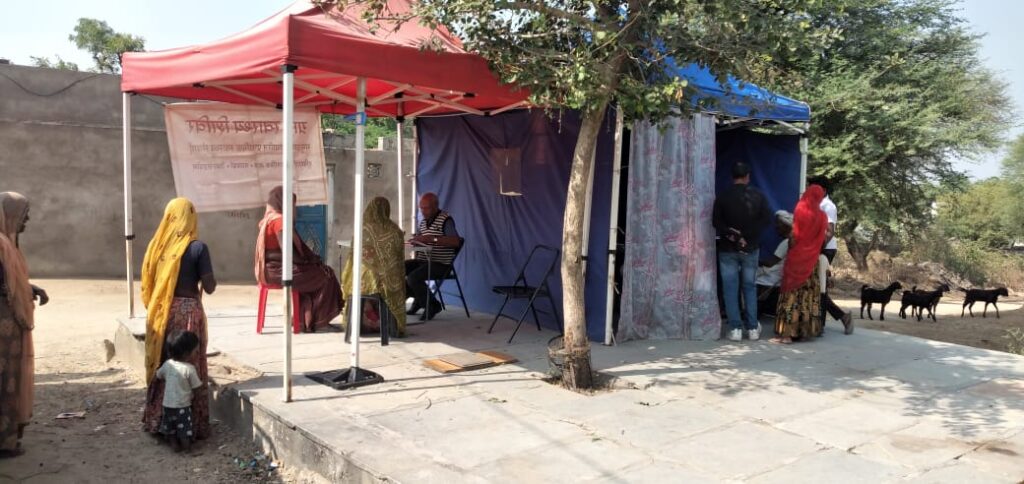
With the advent of COVID-19, access to health care, especially for chronic diseases suffered as government resources were increasingly diverted towards control of COVID-19. Therefore in June 2020 we initiated tent-based monthly health camps to provide primary health care to vulnerable families living in interior rural and tribal areas of southern Rajasthan. The camps were set up specifically to minimize the risk of spread of the virus – they were partially open, allowed for greater air circulation, and could be set up or dismantled within 20 minutes. In the first phase we organized two half-day camps on each day in different villages, and later in the second phase in one location on pre-scheduled and publicised days. Now that the pandemic has ebbed, we have started using schools and other government buildings along with tents, to ensure better privacy and protection from inclement weather. The camps now form part of a health care system for older persons and those with chronic diseases, as shown in the accompanying graphic. ARTH’s community health workers identify sick persons, including severely malnourished children and older persons and refer them to the nearest camp. There, a doctor examines them, support staff provides the patient with free medication, mobility aids and explains dosage, diet, exercise, etc. The patient is encouraged to visit again to ensure that treatment is working. Those with chronic conditions in need of specialised investigations or care are referred (expenses paid) to the Government Hospital in Udaipur, where ARTH’s referral navigator meets and accompanies them through tests and outpatient clinics. ARTH’s telephone call centre supports both family and referral navigator to ensure better coordination. Afterwards, patients are encouraged to follow up at subsequent camps, some are referred to the local primary health centre for continuing access to free drugs. We are also beginning to connect to recently established Health & Wellness Centres. Thus our health camps therefore have become a link for enabling the community to access different levels of health care for chronic diseases. From June 2020 to March 2023, ARTH has conducted 345 monthly camps with a footfall of 4,459 persons, of which 28% were senior citizens. Major chronic conditions being treated through these camps include hypertension, malnutrition, diabetes and COPD. We see periodic camps at the same location as representing a hybrid service delivery mechanism, between ad hoc or one-shot health camps and fixed facilities. They have greater relevance for interior areas and under-served communities that carry a heavier burden of undetected or untreated chronic morbidity.
Reproductive & child health centres (1997 onwards)

ARTH has been providing RCH services in its field area through three rural health centres at Iswal, Lakmawato ka Guda and Suawaton ka Guda. At Urban health clinic and Paneriyo ki Bhagal Clinic, nurse midwives provide RCH services from 9 am to 5 pm 6 days a week with weekly visits by gynaecologists. At rural health clinics centres, nurse-midwives provide RCH services and emergency services round the clock. A gynaecologist visits the centres once a week. The RCH services provided at the health centres include : ARTH’s trained nurse-midwives use a Basic Model of Midwifery and provide a wide range of maternal-neonatal services and managing complications in the absence of a doctor. An active system of referral (counselling for decision making, arranging transport, accompanying the patient till referral hospital) allows the majority of patients to receive emergency care for complications.
First trimester abortion services (1999 onwards)

Many women who carried the burden of unwanted pregnancies, went to the informal service providers, often with disastrous consequences. There were no certified abortion facilities in the block when ARTH started its work. Given the need, ARTH decided to start the provision of safe abortion services. ARTH’s clinical facilities were certified by the State Government in December 1999. A gynaecologist visits the centres on fixed days once a week from 10 AM to 4 PM throughout the year. First trimester MTP services are provided during those fixed days using medical abortion drugs. A trained paramedic/nurse midwife acts as a back-up to address post MTP complications, if any. Two nurse midwives have a role in pre-MTP counselling, screening and follow up after the procedure. ARTH’s health centres do not insist that women who seek abortions services bring their husbands or another attendant with them. This is especially crucial to women because of high rates of migration of men from the area. Men visit the villages periodically, and wives often come to know about their pregnancy after the husband has gone back to the city. Till September 2024, ARTH’s centres have provided MTPs to 15,488 women. The proportion of women seeking medical abortion has been steadily increasing over the last few years. The safe abortion services provided by ARTH demonstrate that it is feasible to provide first trimester abortions in rural interiors with a system of visiting doctors and locally resident nurse-midwives, using MVA and/or medical abortion.
Home Care – (2018 – 2021)

Integrating clinical and home care for mother, infants and introducing services for mental health and care of older persons Overview Home Care was an initiative to provide a continuum of care extending from home to hospitals for rural – tribal women, infants, older persons and persons with psychosocial problems, in over 150,000 population in southern Rajasthan, India. Local youth (men and women) were trained and deployed as Home Care Workers to serve their community. They visited homes, surveyed, screened, identified and/ or provided supervised care using point of care equipment, and referred those needing clinical work up to clinics and hospitals. Programme Details Expected Outcomes Results Over a span of three years, we screened 4,532 older persons. Of these, 3,271 (72%) were identified as having a health problem and were advised referral to a health facility for further treatment. Of those referred, 1,367 (42%) of them went for treatment at least once at an ARTH Camp, clinic, or via telemedicine. A few older persons appeared to be willing to learn about maintenance of their functional abilities, but the larger group was looking for quick solutions to their long-term health problems. Most older persons presented with multiple morbidities and at times required further assessment at a higher centre. We referred and tried to connect them with specialists, but they were reluctant to go due to fear of COVID-19 – families believed that they would be admitted and isolated if they went to district hospitals. Some older persons opted to visit private practitioners in the city or in neighbouring towns. With the advent of COVID-19, we had to pivot in order to provide treatment, especially for those with chronic illnesses. Therefore we started conducting tent-based camps (which could be set up and dismantled in 20 mins), to minimise the risk of indoor infection. We also stopped group mobilisation and started reaching out to individuals, especially those living in remote areas.
Continuum of Maternal-Neonatal-Infant Care (2007-2011)

India used to witness the largest number of maternal deaths in any single country, and within India, Rajasthan had among the highest maternal death rates. The early postpartum period has been recognized to be a time of heightened risk for both mother and newborn. While significant progress has occurred in developing community based approaches for promoting neonatal health, similar attention had not been paid to improving maternal health during the postpartum period. Project Objectives: Strategy/Approach: Progress/Outcomes: The initial results of the study shed light on the terminology used by women to describe their postpartum morbidities and proved useful to further develop communication messages. It also showed that some life threatening morbidities continue to affect women beyond the 42 day period, in the first year after childbirth and hence it was important to provide care for one year after delivery. The study was extended twice beyond its initial 3 years (2006-2009) in order to include further intervention time (2009-2010) as well as to complete an endline survey (2010-2011) and data analysis. Perinatal mortality rates, as mentioned earlier, declined overall throughout the duration of this project and as the intervention continued. While there were many fluctuations up and down when examined by location of delivery, the one exception that has spiked rather than declined has been in the case of home births where the rate dropped from 77.1 in 2008 to 59.1 in 2011 and sprang up again to 104.7 in 2012. Similarly, there was an overall decline in the neonatal mortality rate (including early and late neonatal mortality rates), but only a very small dip (around 1.5%) in the stillbirth rate in the ARTH field area over the course of the project. The timings of postnatal maternal deaths also fluctuated, with a gradual decline in early postpartum maternal death (<24 hours after delivery) by 50%. This is significant because it points to an increase in the amount of time women stayed in the birthing facilities and received more and improved care. Overall, there were positive maternal and neonatal health outcomes as a result of increased reporting of delivery by medical and local informants, and postnatal care by nurse-midwives. Click here for detailed information
Gaon Pas” : Village pregnancy advisory services (2007-2010)

“Gaon Pas” : Village pregnancy advisory services (2007-2010) In July 2007, ARTH introduced village level pregnancy advisory services. This effort utilised the potential of non-medical persons (ASHAs) to increase awareness of and access to reproductive health services to enable women to better manage their own fertility. The key components of the initiative were: Click here for detailed information
Copper-T 380A as an alternative to female sterilization (1999-2004)

One of ARTH’s successful innovations has been the introduction of Copper-T 380A (the “ten year Copper-T”) in the community. ARTH undertook social marketing of 10 year Copper-T as a reversible alternative to sterilization. The Ten year Copper-T is being offered since July 1998, by the gynecologists’ and nurse midwives. The intervention of 10 year Copper T questioned many of the straitjacketed assumptions on adoption of family planning. Some of the key lessons were :
Self-help groups for improving RCH (2003 – 2008)

In 2003, ARTH formed women self-help groups, with the aim of organising communities for improving their access to health care. ARTH formed a total of 105 SHGs in the field area. Using SHGs’ social network as a community health platform, ARTH attempted to enhance people’s access to health care. 5 key strategies to support health care through SHGs were used: